In this paper, a deterministic mathematical model illustrating the transmission dynamics of pulmonary tuberculosis and pneumonia co-infection is formulated, incorporating a drug-resistant strain. The model employs a Holling-type functional response to capture the impact of natural immunity on the progression from latent tuberculosis infection to active disease, as well as its role in controlling drug-resistant pulmonary tuberculosis-pneumonia co-infections. The model is extended to include optimal control theory, aimed at identifying strategies to minimize co-infections using prevention, screening of latently infected individuals, and treatment as control variables. Pontryagin’s Maximum Principle is applied to characterize the optimal control system. The resulting optimality system is then solved numerically using the Runge-Kutta-based forward-backward sweep method. Numerical simulations demonstrate that enhancing natural immunity among latently infected individuals significantly reduces the number of co-infected cases. The optimal control analysis indicates that the most effective strategy for controlling or reducing co-infections of drug-resistant tuberculosis and pneumonia is the combined optimization of infection prevention and screening of latently infected individuals. These findings underscore the importance of scaling up preventive measures against pulmonary tuberculosis and opportunistic pneumonia, alongside screening efforts, to effectively control co-infections. Additionally, the study recommends strengthening immunity among latently infected populations to further reduce the prevalence of co-infections.
| Published in | American Journal of Mathematical and Computer Modelling (Volume 10, Issue 4) |
| DOI | 10.11648/j.ajmcm.20251004.12 |
| Page(s) | 121-144 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Pulmonary Tuberculosis, Co-infection, Latently Infected, Natural Immunity, Drug-resistant Strain, Optimal Control
Variable | Definition |
|---|---|
| Individuals susceptible to pulmonary tuberculosis |
| Individuals vaccinated against pulmonary tuberculosis |
| Individuals latently infected with the drug-sensitive strain of pulmonary TB |
| Individuals latently infected with the drug-resistant strain of pulmonary TB |
| Individuals infected with the drug-sensitive strain of pulmonary tuberculosis |
| Individuals infected with the drug-resistant strain of pulmonary tuberculosis |
| Individuals co-infected with the drug-sensitive strain of TB and pneumonia |
| Individuals co-infected with the drug-resistant strain of TB and pneumonia |
| Individuals undergoing treatment for the drug-sensitive strain of pulmonary TB |
| Individuals undergoing treatment for the drug-resistant strain of pulmonary TB |
| Individuals undergoing treatment for co-infection with the drug-sensitive strain of pulmonary TB and pneumonia |
| Individuals undergoing treatment for co-infection with the drug-resistant strain of pulmonary TB and pneumonia |
| Individuals who have recovered |
Parameter | Description |
|---|---|
Recruitment rate of individuals into the population. | |
Proportion of the population that is vaccinated. | |
Efficacy of the pulmonary tuberculosis vaccine. | |
, , . | Forces of infection for drug-sensitive tuberculosis, drug-resistant tuberculosis, and pneumonia, respectively. |
| Natural death rate. |
, | Rates at which individuals latently infected with the drug-sensitive and drug-resistant strains of pulmonary TB are screened. |
, | Treatment rates of individuals with drug-sensitive and drug-resistant tuberculosis. |
, . | Rates at which individuals with drug-sensitive and drug-resistant TB-pneumonia co-infection are screened. |
, . | Rates of progression from latent drug-sensitive and drug-resistant strain infections to TB disease. |
, . | Rates at which individuals undergoing treatment for the drug-sensitive strain of TB, and for co-infection with the drug-sensitive strain of TB and pneumonia, respectively, develop a resistant strain. |
, . | Rates at which individuals co-infected with the drug-sensitive and drug-resistant strains of TB and pneumonia recover from acute pneumonia. |
, . | Rates at which individuals co-infected with the drug-sensitive and drug-resistant strains of TB and pneumonia recover from acute pneumonia while undergoing treatment. |
, , , , , , , . | Mortality rates due to the drug-sensitive strain of TB; drug-resistant strain of TB; co-infection with the drug-sensitive strain of TB and pneumonia; co-infection with the drug-resistant strain of TB and pneumonia; drug-sensitive TB in individuals undergoing treatment; drug-resistant TB in individuals undergoing treatment; co-infection with the drug-sensitive strain of TB and pneumonia in individuals receiving treatment; and co-infection with the drug-resistant strain of TB and pneumonia in individuals undergoing treatment, respectively. |
| Rates at which individuals with the drug-sensitive and drug-resistant strains of TB recover while undergoing treatment, respectively. |
| An immunity parameter that delays the progression to severe tuberculosis. |
Rate at which individuals who have recovered from TB become susceptible again | |
, , . | Transmission rates of drug-sensitive TB, drug-resistant TB, and pneumonia, respectively. |
, , , , , . | Transmission coefficients of tuberculosis from: the drug-sensitive TB strain only; co-infection with the drug-sensitive TB strain and pneumonia during treatment; the drug-sensitive TB strain during treatment; the drug-resistant TB strain; co-infection with the drug-resistant TB strain and pneumonia during treatment; and the drug-resistant TB strain only during treatment, respectively. |
, , . | Transmission coefficients of pneumonia from: individuals co-infected with the drug-resistant strain of TB and pneumonia; individuals co-infected with the drug-sensitive strain of TB and pneumonia who are undergoing treatment; and individuals co-infected with the drug-resistant strain of TB and pneumonia during treatment, respectively. |
Parameter | Value | Reference |
|---|---|---|
1508563 | [ 29] | |
0.8 | [ 29] | |
0.6 | [1] | |
0.0057 | [ 29] | |
, | 0.7, 0.3 | [3 0] |
, | 0.6, 0.8 | [3 0] |
, | 0.023, 0.053 | Data fitted |
0.0003 | Data fitted | |
, | 0.006, 0.06 | [3 1] |
0.005 | Data fitted | |
0.03 | Data fitted | |
, | 0.06, 0.007 | [31] |
, | 0.00031, 0.00011 | Data fitted |
, | 0.34,0.05 | [3 1] |
, | 0.75,0.7 | [3 1] |
0.08 | Data fitted | |
| 0.065 | Data fitted |
| 0.035 | Data fitted |
, | 0.001, 0.00219 | Data fitted |
0.003 | [3 2] | |
| [3 1] | |
| [3 1] | |
| [3 1] | |
, | 0.002, 0.003 | Data fitted |
, , | 0.3704, 0.1655, 0.1527 | Data fitted |
, , | 0.1487, 0.1389, 0.1054 | Data fitted |
, , | 0.0315, 0.0576, 0.6012 | Data fitted |
Parameter | Sensitivity index |
|---|---|
Sensitivity indices of | |
| |
| |
| |
| |
| |
| |
| |
| |
+1 | |
Sensitivity indices of | |
| |
| |
| |
| |
| |
| |
| |
+1 |
TB | Tuberculosis |
S | Susceptible |
E | Exposed |
I | Infectious |
R | Recovered |
N | Total Human Population |
| [1] | World Health Organization. (2023). Global tuberculosis report 2023. Retrieved May 10, 2025, from |
| [2] |
World Health Organization. (2024). Tuberculosis fact sheet. Retrieved May 14, 2025, from
https://www.who.int/news-room/fact-sheets/detail/tuberculosis |
| [3] | Garcia, R. (2019). Community‐acquired pneumonia due to Streptococcus pneumoniae: when to consider coinfection with active pulmonary tuberculosis. Case Reports in Infectious Diseases, 2019(1), 4618413. |
| [4] | Chavarría, A. G. C., & Quirós, L. B. (2018). Coinfection with Staphylococcus aureus community-acquired pneumonia and mycobacterium tuberculosis in a diabetic patient: a case report. Int Phys Med Rehab J, 3(3), 262-263. |
| [5] | Yan, P., & Chowell, G. (2019). Quantitative methods for investigating infectious disease outbreaks (Vol. 70). Cham, Switzerland: Springer. |
| [6] | Baguelin, M., Medley, G. F., Nightingale, E. S., O’Reilly, K. M., Rees, E. M., Waterlow, N. R., & Wagner, M. (2020). Tooling-up for infectious disease transmission modelling. Epidemics, 32, 100395. |
| [7] | Kirimi, E. M., Muthuri, G. G., Ngari, C. G., & Karanja, S. (2024). Modeling the effects of vaccine efficacy and rate of vaccination on the transmission of pulmonary tuberculosis. Informatics in Medicine Unlocked, 46, 101470. |
| [8] | Kirimi, E. M., Muthuri, G. G., Ngari, C. G., & Karanja, S. (2024). A Model for the Propagation and Control of Pulmonary Tuberculosis Disease in Kenya. Discrete Dynamics in Nature and Society, 2024(1), 5883142. |
| [9] | Li, Q., & Wang, F. (2023). An epidemiological model for tuberculosis considering environmental transmission and reinfection. Mathematics, 11(11), 2423. |
| [10] | Alfiniyah, C., Soetjianto, W. S. P. A., Aziz, M. H. N., & Ghadzi, S. M. B. S. (2024). Mathematical modeling and optimal control of tuberculosis spread among smokers with case detection. AIMS Mathematics, 9(11), 30472-30492. |
| [11] | Xu, C., Cheng, K., Guo, S., Yuan, D., & Zhao, X. (2024). A dynamic model to study the potential TB infections and assessment of control strategies in China. arXiv preprint arXiv: 2401.12462. |
| [12] | Ochieng, F. O. (2025). SEIRS model for TB transmission dynamics incorporating the environment and optimal control. BMC Infectious Diseases, 25(1), 490. |
| [13] | Kang, T. L., Huo, H. F., & Xiang, H. (2024). Dynamics and optimal control of tuberculosis model with the combined effects of vaccination, treatment and contaminated environments. Mathematical Biosciences and Engineering, 21(4), 5308-5334. |
| [14] | Otoo, D., Osman, S., Poku, S. A., & Donkoh, E. K. (2021). Dynamics of Tuberculosis (TB) with Drug Resistance to First‐Line Treatment and Leaky Vaccination: A Deterministic Modelling Perspective. Computational and Mathematical Methods in Medicine, 2021(1), 5593864. |
| [15] | Mengistu, A. K., & Witbooi, P. J. (2023). Cost‐Effectiveness Analysis of the Optimal Control Strategies for Multidrug‐Resistant Tuberculosis Transmission in Ethiopia. International Journal of Differential Equations, 2023(1), 8822433. |
| [16] | Aldila, D., Awdinda, N., Herdicho, F. F., Ndii, M. Z., & Chukwu, C. W. (2023). Optimal control of pneumonia transmission model with seasonal factor: learning from Jakarta incidence data. Heliyon, 9(7). |
| [17] | Yano, T. K., & Bitok, J. (2022). Computational Modelling of Pneumonia Disease Transmission Dynamics with Optimal Control Analysis. Appl. Comput. Math, 11(5), 130-139. |
| [18] | Swai, M. C., Shaban, N., & Marijani, T. (2021). Optimal control in two strain pneumonia transmission dynamics. Journal of Applied Mathematics, 2021(1), 8835918. |
| [19] | Legesse, F. M., Rao, K. P., & Keno, T. D. (2023). Cost effectiveness and optimal control analysis for bimodal pneumonia dynamics with the effect of children's breastfeeding. Frontiers in Applied Mathematics and Statistics, 9, 1224891. |
| [20] |
World Health Organization. (2025). Integrated approach to tuberculosis and lung health: Policy brief. Geneva: World Health Organization. Licence: CC BY-NC-SA 3.0 IGO. Retrieved May 14, 2025, from
https://iris.who.int/bitstream/handle/10665/380840/9789240107526-eng.pdf%20?Sequence =1 |
| [21] | Gweryina, R. I., Madubueze, C. E., Bajiya, V. P., & Esla, F. E. (2023). Modeling and analysis of tuberculosis and pneumonia co-infection dynamics with cost-effective strategies. Results in Control and Optimization, 10, 100210. |
| [22] | Xiao- Ying, L., Hong- fei, D., Li-mei, Y., & Wei-min, L. (2016). Pulmonary tuberculosis and bacterial pneumonia co-infection; a clinical etiology investigation in China. Chinese Journal of Zoonoses, 30 (4), 364-372. |
| [23] | Chandra, P., Grigsby, S. J., & Philips, J. A. (2022). Immune evasion and provocation by Mycobacterium tuberculosis. Nature Reviews Microbiology, 20(12), 750-766. |
| [24] | Banerjee, S. (2021). Mathematical modeling: models, analysis and applications. Chapman and Hall/CRC. |
| [25] | Khajanchi, S., Das, D. K., & Kar, T. K. (2018). Dynamics of tuberculosis transmission with exogenous reinfections and endogenous reactivation. Physica A: Statistical Mechanics and its Applications, 497, 52-71. |
| [26] | Driessche, K., Khajanchi, S., & Kar, T. K. (2020). Transmission dynamics of tuberculosis with multiple re-infections. Chaos, Solitons & Fractals, 130, 109450. |
| [27] | Khajanchi, S., Bera, S., & Roy, T. K. (2021). Mathematical analysis of the global dynamics of a HTLV-I infection model, considering the role of cytotoxic T-lymphocytes. Mathematics and Computers in Simulation, 180, 354-378. |
| [28] | Chowell, G., & Kiskowski, M. (2016). Modeling ring-vaccination strategies to control Ebola virus disease epidemics. Mathematical and statistical modeling for emerging and re-emerging infectious diseases, 71-87. |
| [29] |
KNBS 2023. Statistical Abstract 2023. Nairobi, Kenya. Retrieved May 21, 2025, from
https://www.knbs.or.ke/wp-content/uploads/2023/11/2023-Statistical-Abstract.pdf |
| [30] |
National Tuberculosis, Leprosy and Lung Disease Program. National strategic plan for tuberculosis, leprosy and lung health 2019-2023. Ministry of Health, Kenya. Retrieved May 23, 2025, from
https://nltp.co.ke/wp-content/uploads/2020/12/National-Strategic-Plan-2019-2023.pdf |
| [31] | National Tuberculosis, Leprosy and Lung Disease Program. 2022 Annual Report. Ministry of Health, Kenya. Retrieved May 21, 2025, from |
| [32] | National Tuberculosis, Leprosy and Lung Disease Program. 2023 Annual Report. Ministry of Health, Kenya. Retrieved May 21, 2025, from https://nltp.co.ke/wp-content/uploads /2025/ 03/2023-Annual-Report.pdf |
| [33] | Obsu, L. L. (2022). Optimal control analysis of a tuberculosis model. Journal of Biological Systems, 30(04), 837-855. |
APA Style
Kirimi, E. M., Okelo, J., Kimathi, M., Ngure, K. (2025). Modeling Pulmonary Tuberculosis-Pneumonia Co-dynamics Incorporating Drug Resistance with Optimal Control. American Journal of Mathematical and Computer Modelling, 10(4), 121-144. https://doi.org/10.11648/j.ajmcm.20251004.12
ACS Style
Kirimi, E. M.; Okelo, J.; Kimathi, M.; Ngure, K. Modeling Pulmonary Tuberculosis-Pneumonia Co-dynamics Incorporating Drug Resistance with Optimal Control. Am. J. Math. Comput. Model. 2025, 10(4), 121-144. doi: 10.11648/j.ajmcm.20251004.12
AMA Style
Kirimi EM, Okelo J, Kimathi M, Ngure K. Modeling Pulmonary Tuberculosis-Pneumonia Co-dynamics Incorporating Drug Resistance with Optimal Control. Am J Math Comput Model. 2025;10(4):121-144. doi: 10.11648/j.ajmcm.20251004.12
@article{10.11648/j.ajmcm.20251004.12,
author = {Erick Mutwiri Kirimi and Jeconiah Okelo and Mark Kimathi and Kenneth Ngure},
title = {Modeling Pulmonary Tuberculosis-Pneumonia Co-dynamics Incorporating Drug Resistance with Optimal Control
},
journal = {American Journal of Mathematical and Computer Modelling},
volume = {10},
number = {4},
pages = {121-144},
doi = {10.11648/j.ajmcm.20251004.12},
url = {https://doi.org/10.11648/j.ajmcm.20251004.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajmcm.20251004.12},
abstract = {In this paper, a deterministic mathematical model illustrating the transmission dynamics of pulmonary tuberculosis and pneumonia co-infection is formulated, incorporating a drug-resistant strain. The model employs a Holling-type functional response to capture the impact of natural immunity on the progression from latent tuberculosis infection to active disease, as well as its role in controlling drug-resistant pulmonary tuberculosis-pneumonia co-infections. The model is extended to include optimal control theory, aimed at identifying strategies to minimize co-infections using prevention, screening of latently infected individuals, and treatment as control variables. Pontryagin’s Maximum Principle is applied to characterize the optimal control system. The resulting optimality system is then solved numerically using the Runge-Kutta-based forward-backward sweep method. Numerical simulations demonstrate that enhancing natural immunity among latently infected individuals significantly reduces the number of co-infected cases. The optimal control analysis indicates that the most effective strategy for controlling or reducing co-infections of drug-resistant tuberculosis and pneumonia is the combined optimization of infection prevention and screening of latently infected individuals. These findings underscore the importance of scaling up preventive measures against pulmonary tuberculosis and opportunistic pneumonia, alongside screening efforts, to effectively control co-infections. Additionally, the study recommends strengthening immunity among latently infected populations to further reduce the prevalence of co-infections.
},
year = {2025}
}
TY - JOUR T1 - Modeling Pulmonary Tuberculosis-Pneumonia Co-dynamics Incorporating Drug Resistance with Optimal Control AU - Erick Mutwiri Kirimi AU - Jeconiah Okelo AU - Mark Kimathi AU - Kenneth Ngure Y1 - 2025/10/14 PY - 2025 N1 - https://doi.org/10.11648/j.ajmcm.20251004.12 DO - 10.11648/j.ajmcm.20251004.12 T2 - American Journal of Mathematical and Computer Modelling JF - American Journal of Mathematical and Computer Modelling JO - American Journal of Mathematical and Computer Modelling SP - 121 EP - 144 PB - Science Publishing Group SN - 2578-8280 UR - https://doi.org/10.11648/j.ajmcm.20251004.12 AB - In this paper, a deterministic mathematical model illustrating the transmission dynamics of pulmonary tuberculosis and pneumonia co-infection is formulated, incorporating a drug-resistant strain. The model employs a Holling-type functional response to capture the impact of natural immunity on the progression from latent tuberculosis infection to active disease, as well as its role in controlling drug-resistant pulmonary tuberculosis-pneumonia co-infections. The model is extended to include optimal control theory, aimed at identifying strategies to minimize co-infections using prevention, screening of latently infected individuals, and treatment as control variables. Pontryagin’s Maximum Principle is applied to characterize the optimal control system. The resulting optimality system is then solved numerically using the Runge-Kutta-based forward-backward sweep method. Numerical simulations demonstrate that enhancing natural immunity among latently infected individuals significantly reduces the number of co-infected cases. The optimal control analysis indicates that the most effective strategy for controlling or reducing co-infections of drug-resistant tuberculosis and pneumonia is the combined optimization of infection prevention and screening of latently infected individuals. These findings underscore the importance of scaling up preventive measures against pulmonary tuberculosis and opportunistic pneumonia, alongside screening efforts, to effectively control co-infections. Additionally, the study recommends strengthening immunity among latently infected populations to further reduce the prevalence of co-infections. VL - 10 IS - 4 ER -
Department of Mathematics, Pan African University Institute for Basic Sciences, Technology, and Innovation, Nairobi, Kenya
Department of Pure and Applied Mathematics, Jomo Kenyatta University of Agriculture and Technology, Nairobi, Kenya
Department of Mathematics and Statistics, Machakos University, Machakos, Kenya
Department of Public and Community Health, Jomo Kenyatta University of Agriculture and Technology, Nairobi, Kenya
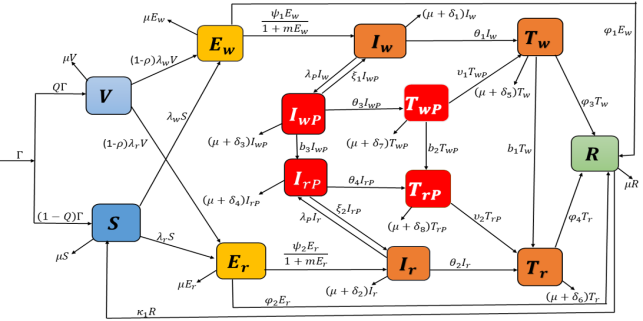
Figure 1. Schematic diagram illustrating the transmission dynamics of pulmonary tuberculosis and pneumonia co-infection incorporating a drug-resistant strain.
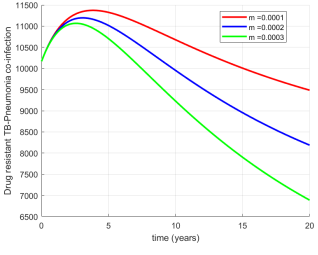
Figure 2. Effects of varying the immunity parameter (m) on drug-resistant tuberculosis-pneumonia co-infections.
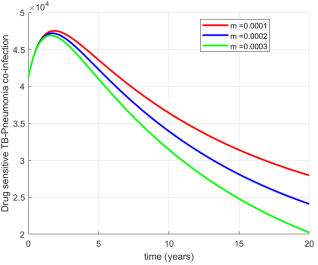
Figure 3. Effects of varying the immunity parameter (m) on drug-sensitive tuberculosis-pneumonia co-infections.
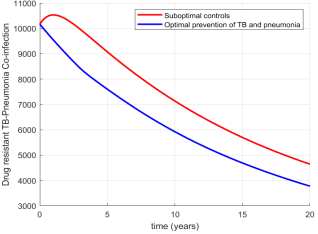
Figure 4. Effects of optimizing prevention on drug-resistant tuberculosis-pneumonia co-infections.
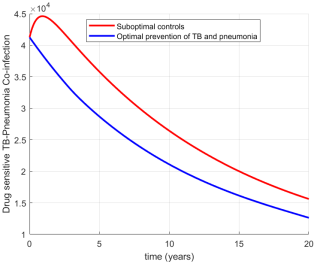
Figure 5.
Effects of optimizing prevention on drug-sensitive tuberculosis-pneumonia co-infections.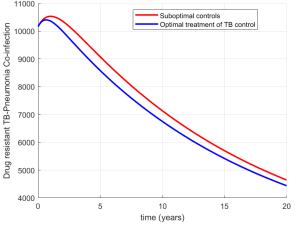
Figure 6. Effects of optimizing treatment on drug-resistant tuberculosis-pneumonia co-infections.
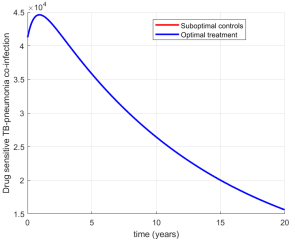
Figure 7. Effects of optimizing prevention on drug sensitive tuberculosis-pneumonia co-infections.
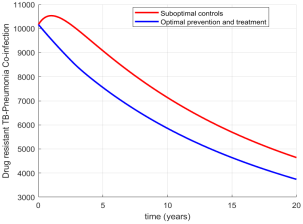
Figure 8. Effects of optimizing prevention and treatment on drug-resistant tuberculosis-pneumonia co-infections.
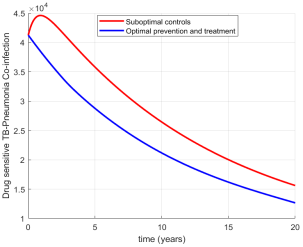
Figure 9. Effects of optimizing prevention and treatment on drug-sensitive tuberculosis-pneumonia co-infections.
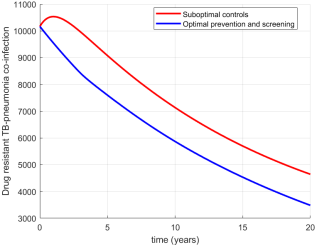
Figure 10. Effects of optimizing prevention and screening on drug-resistant tuberculosis-pneumonia co-infections.
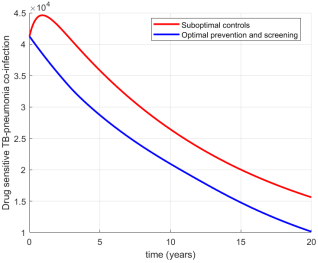
Figure 11. Effects of optimizing prevention and screening on drug-sensitive tuberculosis-pneumonia co-infections.
Information

